

Introduction of CAR-T Therapy
T lymphocytes are engineered with synthetic receptors known as chimeric antigen receptors (CAR) in CAR-T Cell therapy. The CAR-T cell is an effector T cell that recognizes and eliminates specific cancer cells, independent of major histocompatibility complex molecules. (Zhai et al. 2018). Chimeric antigen receptors (CARs) cells have recombinant receptor constructs expressed in T cells to target cells expressing specific antigens.
CAR-T therapy was developed with the construction of recombinant TcRs that replaced the TcR V regions with antigen-specific antibody V regions. The chimeric TcRs retained the normal extracellular C region, the transmembrane segment, and the cytoplasmic signaling domains, and therefore maintained the ability to induce T-cell proliferation, interleukin production, and cell lysis. Furthermore, these chimeric TcRs were non-MHC-restricted and universal in the sense that a given chimeric construct could be transfected into T-cells from any individual, and these transfected cells infused back into the patient to identify and attack cancer cells expressing the target antigen. T cells expressing CAR have been shown to recognize a wide range of surface antigens, including glycolipids, carbohydrate moieties, and proteins (Morello et. al., 2016), and can attack malignant cells expressing these antigens.
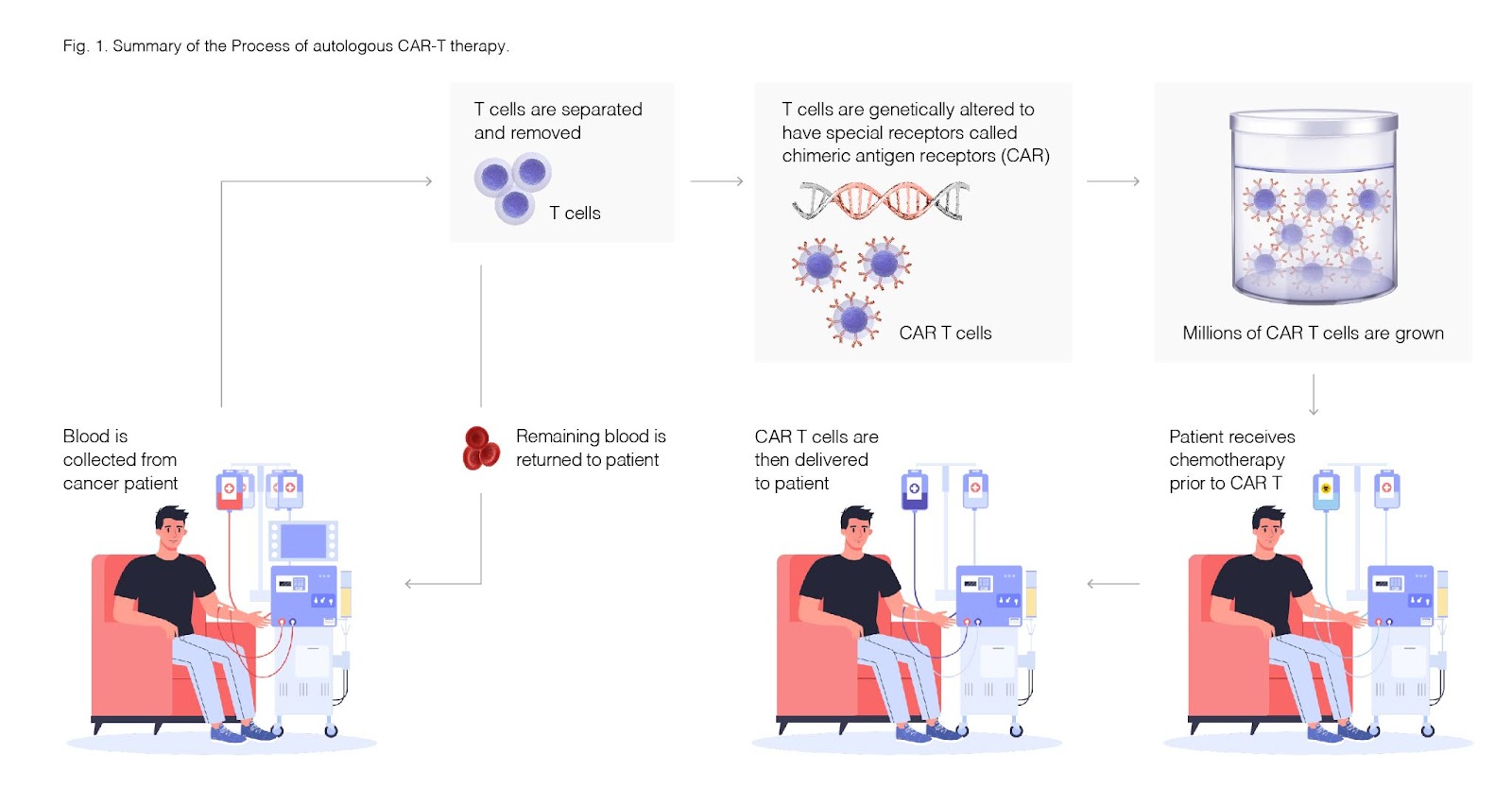
Fig. 1. Summary of the Process of autologous CAR-T therapy.
Types of CAR-T Developed for Therapeutic Applications
CAR-T therapy can be from the patient (autologous) and a donor (allogeneic). In both cases, transforming these normal T cells into CAR-T cells that target specific markers requires the delivery of genetic instructions into these cells, most commonly via viral vectors, but, more recently, genome editing tools CRISPR-Cas9 have also begun to be used.
CAR-T cell approaches have revolutionized cancer therapeutics’ landscape, particularly against hematological malignancies, and remain the most promising approach for treating many types of cancers.
CAR-T cells are simple to construct and customize, which makes them very attractive cell therapy. Several CAR-T product therapies are under clinical development and hold a promising future. The evaluation of side effects of CAR-T therapies and post patient monitoring are two key aspects in developing and commercializing new CAR-T therapies. Post-CAR-T patient monitoring is critical to monitor CAR-T therapy’s success or mitigate side effects of CAR-T Therapy. Availability of Post CAR-T patient monitoring will help to develop/optimize CAR-T therapies.
Patient Monitoring Post-CAR T Therapy using flow cytometry.
A single therapeutic dose of CAR-T contains a target dose of 2×106 CAR-positive viable T cells per kg of body weight, prepared in a volume of 68mL. Before administering the CAR-T cell infusion, the patients undergo lymphodepletion using fludarabine and cyclophosphamide over three days. This is essential for the depletion of endogenous lymphocytes and for the elevation of the homeostatic cytokines IL-15 and IL-7. Two days later, the patient is ready to receive the CAR-T infusion and the patient remains under surveillance for the next 12 days during which Tocilizumab must be immediately available in case of CRS. In addition to monitoring for signs of infection, Cytokine Release Syndrome or neural toxicity, daily hematology and chemical lab tests are performed to track levels of CRP and ferritin, and since atypical lymphocytes that mimic blasts are often associated with the peak of CAR-T expansion, flow cytometry is used to exclude relapse and monitor blood cell counts. Trillium Diagnostics developed a flow cytometry kit, Leuko64, to measure neutrophil CD64 expression as an indicator of infection/sepsis or predictor of severe CRS. The kit can be used as a laboratory-developed test (LDT) within CLIA-certified laboratories. Many other clinical labs have developed flow cytometry-based LDTs to monitor phenotypic changes in leukemia patients following antigen-directed therapies. Such flow cytometry panels can help provide early detection of antigen-escape and Minimal Residual Disease (MRD) in patients, and current recommendations include such testing every 3-6 months for up to 15 years after treatment (Yakoub-Agha et. a. 2020).
The Adoption of Functional Proteomic Profiling of CAR-T Cells
Polyfunctionality of CAR-T-cells can be used as a biomarker of potency, and FlowMetric now offers the Isoplexis platform to support this type of analysis: About 40% of patients taking CAR-T therapy develop severe neurotoxicity’s. Functional profiling, such as that provided by this platform, is a powerful tool in developing safe and effective CAR-T products and in predicting patient outcomes. The Isoplexis technology has been used to characterize neurotoxicity in CAR-T product. Rossi et al (2018) have used IsoPlexis’ single-cell functional immune landscaping technology to identify polyfunctional cells, and performed analysis using IsoPlexis’ Polyfunctional Strength Index (PSI), a unique polyfunctionality metric.This study also highlights CAR-T cell polyfunctionality as a useful metric to predict clinical outcomes. Monitoring CAR-T polyfunctionality may be critical to improving CAR-T efficacy and preventing adverse immune responses. Functional proteomic profiling uniquely addresses current challenges in neuroinflammatory responses, accelerating the development of personalized and targeted therapies.
Proteomic analysis can detect heterogeneous and potent cells within a phenotypically identical sample. IsoPlexis’ single-cell cytokine detection system analyzes the true function of each cell, and enabling up to 40 parameters to be described for each cell.
This type of functional analysis has been used to monitor cellular changes during the development and optimization of CAR-T manufacturing process and in screening for polyfunctionality. This innovative technology offers great potential to improve CAR-T therapies by quantifying and profiling the functionally heterogeneous and potent cells using modified CAR- constructs and within different therapeutic preparations.
Flow cytometry assay at Flowmetric Inc.
Incorporating into the CAR T manufacturing process are several Quality Checkpoints. Rigorous QC testing is performed in batch release tests for T-cell viability and sample purity, T-cell potency in the form of effector function and activation, and microbiological safety.
The robustness of the product quality control process is demonstrated through quality control of the CAR-T product and the preventative/corrective action, change control, and review protocols in place. Release testing frequently involves flow cytometry analysis of the cells to determine the purity of the therapeutic preparation and potency evaluation for different CAR- constructs.
Flowmetric has developed and validated various flow cytometry panels and functional profiling methods for several different CAR-T products. Our team continues to bring online a portfolio of tests to monitor patients pre-, during, and post-treatment as these cellular therapies continue to spearhead the area of targeted precision medicine.
| Authored by: Dr. Sibtain Ahmed |
Dr. Sibtain Ahmed is a scientific writer and a member of FlowMetric’s Business Development team. Sibtain is a skilled a biochemist with experience in the field of biologics, and cell and gene therapy manufacturing, drug discovery, vaccines, and fermentation. Sibtain earned his B.S. in Biology at the University of the Punjab and his Ph.D. from the University of Agriculture Faisalabad. Sibtain did postdoc research at the University of New Mexico and the University of California San Diego. Sibtain’s previous work history includes working at Thermo Fisher Scientific, Hologic, and the Genomics Institute of the Novartis Research Foundation. Sibtain has authored peer-reviewed articles/book chapters, presented posters, and has given oral talks in
scientific meetings.
References
Zhao Z, Chen Y, Francisco NM, Zhang Y, Wu M. 2018. The application of CAR-T cell therapy in hematological malignancies: advantages and challenges. Acta Pharm Sin B. Jul;8(4):539-551. doi: 10.1016/j.apsb.2018.03.001.
Demaret J, Varlet P, Trauet J, Beauvais D, Grossemy A, et al..2020. Monitoring CAR T‐cells using flow cytometry. Cytometry Part B: Clinical Cytometry. doi: 10.1002/cyto.b.21941. Epub ahead of print. PMID: 32841511.
Morello A, Sadelain M, Adusumilli PS. (2016) Mesothelin-targeted CARs: driving T cells to solid tumors. Cancer Discov. 6:133–46. DOI: 10.1158/2159-8290.CD-15-0583
Yakoub-Agha I, Chabannon C, Bader P, Basak GW, Bonig H, et al. (2020) Management of adults and children undergoing chimeric antigen receptor T-cell therapy: best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Haematologica 105(2) 297-316.DOI: 10.3324/haematol.2019.229781
Rossi J, Paczkowski P, Shen YW, Morse K, Flynn B. et al. 2018. Preinfusion polyfunctional anti-CD19 chimeric antigen receptor T cells are associated with clinical outcomes in NHL. Blood 2018; 132 (8): 804–814. DOI: 10.1182/blood-2018-01-828343